
 Linfield’s current students are the first to come of age in a time of legal marijuana. What does that mean for campus life?
Linfield’s current students are the first to come of age in a time of legal marijuana. What does that mean for campus life?
By Eric Fetters-Walp ’93
Resident assistants like Kendall Harrison ’21 aren’t focused on busting students who violate Linfield’s alcohol and drug policy, despite what their peers might think. But sometimes they can’t ignore what they see, hear or smell — including the pungent odor of marijuana being smoked inside a residence hall.
“We’re not looking to get students in trouble; we’re looking out for their safety,” Harrison said. “But when we’re out on rounds around campus, marijuana of course is more noticeable than alcohol.”
And RAs are reporting an increase of marijuana-related incidents compared to alcohol-related ones these days, though there still are more alcohol incidents overall. Compared to even a couple years ago, Harrison said, students seem to be less cautious about getting caught with the drug.
The first generation of students to attend college in the era of legalized marijuana is finding the old rules about pot consumption haven’t changed much on campus, including at Linfield. That’s partly because state and federal laws don’t align, and partly because colleges are concerned about the safety and health of their communities.
A complex legal picture
Nearly five years ago, Oregon made it legal for people 21 and older to use marijuana not just for medical reasons, but also for recreation. While our state has seen a boom in cannabis-related businesses — with dispensaries popping up in communities from the coast to the Wallowas — it’s still illegal for most students because they’re underage. And there’s another big barrier: The federal Drug Enforcement Administration still classifies marijuana as a Schedule I drug, meaning it’s a controlled substance with high potential for abuse. For those reasons, marijuana use and possession isn’t allowed on Linfield campuses, said Jeff Mackay ’88, the university’s dean of students. “Our policy is no different than before. It has not changed because the federal law hasn’t changed.”
Linfield’s stance is similar to that of most colleges, public and private, said John Hudak, a Brookings Institution senior fellow and author of the book Marijuana: A Short History.
“There are a lot of challenges that schools face on this,” he said. “Some of those challenges are historical, some have to do with public relations and some are legal.”
Because the federal government classifies marijuana as an illegal drug, a 1989 law known as the Drug-Free Schools and Communities Act requires that colleges and universities prohibit it. If they don’t, schools could lose access to federally funded student loan and grant programs, research money and more.
And most college leaders have long fought to reduce underage students’ use of alcohol and drugs, not just to comply with federal law, but also to increase campus health and safety. Partially changing that stance isn’t appetizing to trustees and college presidents, Hudak said. It probably would not thrill a large number of parents, either.
Like alcohol, but different
Linfield’s student policy guide specifies that any member of the university community who uses or possesses drugs, including “marijuana, marijuana oil, food products, etc.,” is subject to disciplinary action. The policy, Mackay said, treats students who break it just like students who run afoul of the campus rules on alcohol use.
Because of the conflict between state and federal laws, he said, new students are informed about the school policy at orientation and again by resident assistants. “When a student decides to come to Linfield, they’re technically supposed to know about it from reading the student handbook,” said Harrison, the RA. “But if they don’t, we also go over it when they arrive on campus.”
It takes some explaining since the rules on marijuana and alcohol use differ. Because it’s legal nationwide to drink at 21, students over that age are allowed to drink on campus. But the same isn’t true for marijuana.
The number of students caught violating the marijuana-use policy has steadily increased in recent years, Mackay said. That falls in line with a recent Oregon State University study that found increased use of marijuana among college students is more noticeable in states where recreational use is legal.
Eleven states, including Oregon, Washington and California, currently allow recreational use. Students in states where the drug is legal were 18% more likely to have used marijuana in the past 30 days than students in other states, the OSU study found. It also found that binge drinking on campuses, a longtime problem combatted by college officials, decreased faster in states with legal marijuana.
The road ahead
For many reasons, including the funding issues at stake, Hudak predicts most colleges will maintain strict rules about marijuana, even as more states make it legal for adults. “There’s reason to believe that even in the face of broader legalization many colleges will continue to have outright bans,” he said.
Even if federal law didn’t effectively make pot illegal on campus, one concern is that allowing older students to use the drug would inevitably make it more accessible to underage students. There are also questions about how it could be used on campus grounds and buildings. Consider student residences, Hudak said. Tobacco use is not allowed inside publicly accessible buildings, including dorms. Smoking is also somewhat restricted outdoors on most campuses, including Linfield’s. So allowing students to smoke marijuana would conflict with smoke-free regulations.
Even so, Mackay said that he and other university leaders realize that telling students to just say “no” isn’t effective. One strategy he uses is emphasizing that while it’s legal for adults off campus, marijuana use isn’t compatible with many students’ activities and future career plans.
For example, student-athletes risk their playing status, and student leaders can lose their positions if they are caught using marijuana. Those studying for careers in nursing can expect hospitals to require random drug tests for employees. Students caught violating the marijuana policy are reminded that the long-term health effects of marijuana aren’t thoroughly known.
“We want students to make their own informed decisions,” Mackay said. “So the response from us really focuses on educating them.”
Linfield’s stance is similar to that of most colleges, public and private. “There are a lot of challenges that schools face on this. Some of those challenges are historical, some have to do with public relations and some are legal.”
– John Hudak, Brookings Institution senior fellow
Faculty Perspective
Is marijuana the best medicine?
Long before pot became legal for recreational use, certain states legalized it for medical use. But is cannabis really effective as medicine? Kim Dupree Jones, Ph.D., RN, FNP, FAAN, professor and dean of the Linfield School of Nursing, focuses on just that question in her research.
Jones is also sought after as a nationwide speaker about how cannabis, the plant from which hemp and marijuana are derived, can be used to treat chronic pain.
In a wide-ranging conversation, she shares her expert opinion about clinical cannabis, a.k.a. medical marijuana.
What is in cannabis?
Cannabis is a plant with more than 140 known chemical compounds. Most scientists believe there are many more.
The two best-studied compounds in cannabis are delta-9-tetrahydrocannabinol (THC) and cannabidiol (CBD). Broadly speaking, THC is responsible for the intoxicating effect associated with cannabis and may contribute to therapeutic benefits. CBD is minimally or not intoxicating and may buffer the effects of THC.
In the United States, cannabis is considered a Schedule I substance, which the Drug Enforcement Administration defines as having no currently accepted medical use and a high potential for abuse.
In Oregon, how can cannabis be used as medicine?
Cannabis is available recreationally in Oregon, so any adult can try it. Unlike recreational cannabis, medical cannabis isn’t subject to taxes when you buy it.
In Oregon, doctors do not prescribe cannabis. Instead, they complete a form certifying that a patient has a qualifying medical condition.
About 87% of medical cards in Oregon are for chronic or severe pain. Other conditions include cancerous tumors; glaucoma; HIV or AIDS; certain nerve disorders; post-traumatic stress; and any medical condition that causes cachexia (a wasting syndrome), severe pain, severe nausea or certain seizure disorders.
In February, I testified in support of a bill in the Oregon Legislature that would allow nurse practitioners to discuss cannabis with their patients and sign the form confirming their patients’ qualifying conditions.
Is cannabis equally safe and effective for all conditions?
There has been some progress, but we need more clinical studies to determine effectiveness for a range of conditions. Here’s a summary of where the research currently stands:
The FDA recently approved a CBD-only product, Epidiolex, to treat seizures associated with two rare and severe forms of epilepsy. In order to obtain approval, the drug developers needed to show significant results from multiple clinical trials.
Outside the United States, at least 30 countries have approved the use of Sativex, an oral spray with CBD and THC. It has high-level evidence for the treatment of muscle spasticity in multiple sclerosis, but not for halting the progress of the disease.
The next-largest group of evidence is for chronic pain. Most studies are positive, meaning cannabis is effective. However, the amount of relief varies greatly between patients and products. Most people would see mild to moderate pain reduction. Cannabis can be expensive, however, so it may not be the most cost-effective way to treat chronic pain.
Unfortunately, despite great celebrity support, we do not yet have well done clinical trials that focus on CBD only. Therefore, claims that it can ease pain or anxiety and improve sleep, etc., are considered anecdotal.
Additionally, I’m dubious about cannabis as a treatment for glaucoma. We have several FDA-approved drugs that already work well to prevent glaucoma-related blindness.
What is a typical dose of THC?
Dosing is determined by the percentage of THC included, but there is no universally agreed upon dose. A few states have defined a single dose as 5 to 10 mg of THC. However, characteristics of the user influence the effect. That means that it may affect you differently depending on factors such as your age, weight, previous experience with THC and use of other medications or drugs.
In addition, it’s not possible to convert the dose of a pharmaceutical cannabis product to those sold in a dispensary. For example, just because Sativex is formulated in a 1:1 THC/CBD ratio, it doesn’t mean that a 1:1 THC/CBD product in a dispensary can reliably be substituted.
The amount of THC in dispensary products may be much higher than the amount of THC studied in clinical trials. For example, one study found that the median THC to CBD ratio was 36:1. Laboratory confirmation of purity and potency is still evolving, too. One study found that only 17% of product labels in dispensaries were accurate. Nonetheless, cannabis sold in a licensed dispensary is safer and subject to more regulations than cannabis products you can buy online.
What is the difference between sativa and indica?
While these terms are commonly used colloquially to characterize the expected effect of a given product, they are not scientifically grounded.
Sativa products are purported to have energizing, uplifting and creative effects (a “mind high”). Indica products tend to be sedating, and relaxing physically and mentally (a “body high”).
In reality, the degree to which a product will have energizing, intoxicating or relaxing effects is most likely determined by the relative amounts of THC and CBD in the product.
Will any of my prescription drugs interact with cannabis?
Cannabis has the potential to compound the sedative effects of some drugs and increase or decrease the potency of other medications. These include some types of antacids and antibiotics as well as drugs used to treat anxiety, seizures, skin infections, bipolar disorder, Parkinson’s disease, hepatitis C and HIV.
If you’re curious about how THC or CBD interacts with a specific medication, talk to your pharmacist. They are a great resource for questions regarding drug interactions with cannabis.
Is cannabis associated with any harmful effects or behaviors?
Just like with prescription medication, people need to balance the benefit of the drug against the side effects and risks. The acute euphoric effect of inhaling cannabis is well known. There is now growing evidence regarding the potential harms of longer-term cannabis use.
(See graphics on pages 44 and 45 for details.)
What advice do you have for people who are considering clinical cannabis?
Overall, I’m cautiously enthusiastic about the future of cannabis as a medicine. If people want to try cannabis, consider starting with CBD only, or a more balanced THC/CBD product.
If you decide to use it for a medical condition, talk to your health care provider. Generally speaking, cannabis is more often used to manage symptoms rather than control a disease. For example, Sativex may help with muscle spasticity related to multiple sclerosis, but doctors do not think it can change the course of the disease.
I’d also advise people not to use vaporizers until we learn more about the respiratory diseases associated with them. And children and pregnant women should not use cannabis unless they are being cared for by an epilepsy specialist.
I encourage people interested in clinical cannabis to support legislation that promotes the study of the plant, including removing its Schedule I status.
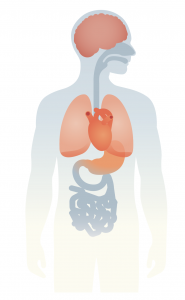 Brain function and mental health
Brain function and mental health
- Cannabis may affect memory, reasoning and perception.
- It may affect brain development in teens and young adults.
- It may increase the risk of mania.
- High-THC products may increase the risk of psychosis symptoms.
Addiction
- One in three people may develop a problematic habit, called cannabis use disorder.
- The degree to which people are affected varies. It may not always rise to the level of addiction.
Withdrawal
- Withdrawal symptoms can last for several weeks.
- Symptoms include moodiness, insomnia, restlessness, chills, anxiety and depression.
- Insomnia is the most common reason for a when trying to quit.
Car accidents
- A cannabis-intoxicated driver is 35% more likely get into an accident.
Lung health
- People who smoke daily may have poorer lung health.
- Regular users have an increased risk of bronchitis.
- Smoking once a week or less is unlikely to affect younger people.
- The effect on older people or people with health conditions is unknown.
Heart rate and blood pressure
- Inhaling cannabis can cause an elevated heart and high or low blood pressure.
- Scientists don’t know yet whether it increases the risk of heart attack or stroke.
Digestion
- Regular users may experience frequent nausea, vomiting and stomach cramps.
- This condition, cannabis hyperemesis syndrome, goes away if you stop using cannabis.
- Warm showers can ease symptoms.
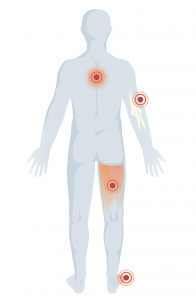 Muscle pain and arthritis
Muscle pain and arthritis
- Cannabis outperforms a placebo, but more research is needed on its effectiveness.
Muscle spasms from multiple sclerosis
- Spasms improved with the short-term use of products with a precise THC/CBD ratio.
- The long-term effects haven’t been studied.
- Effective formulations are often different from those sold at a dispensary.
Chronic pain from disorders
- Products with a precise THC/CBD ratio show promise for short-term pain relief.
- The long-term effects are not clear.
- Effective formulations are often different from those sold at a dispensary.
Data and graphics extracted from Cannabis Provider Education Packet: Evidence Synthesis Program, Portland Veterans Administration.